The maxilla or upper jaw has several qualities that make it unique to grafting as well as the placement of implants. The most significant difference in the maxilla when compared to the mandible lies in the presence of the maxillary sinus. The maxillary sinus is one of the several natural air spaces that are anatomically present in all human skulls (see Figure 6). Its biological purpose is to warm, moisturize and filter air when we breathe. While the maxillary sinus is most often only noticed when one has a cold or infection, it can impose itself on the roots of the teeth in the upper jaw.
As a consequence of this relationship, when a tooth is lost, the result may be the presence of very little bone between the oral cavity and this air space (see Figure 7). In turn, this can make the placement of an implant in the posterior (back) of the upper jaw a slightly bigger project when in comparison to other areas of the jaw. Fortunately, a relatively simple solution has been developed to handle this problem and render a safe, effective and stable result for placing implants. The subantral graft or “sinus lift procedure” has been performed now for many years to allow implants to be used as a replacement for maxillary molars. While some less experienced implant surgeons (periodontists and restorative dentists) are uncomfortable performing this operation to the extent that it is effective, this is a staple procedure for the oral and maxillofacial surgeon. The patient should not fear that this will have an adverse effect on their sinuses or produce chronic sinus pain. Our experience with this procedure is not only vast and longstanding; its use has been commonplace for many years.
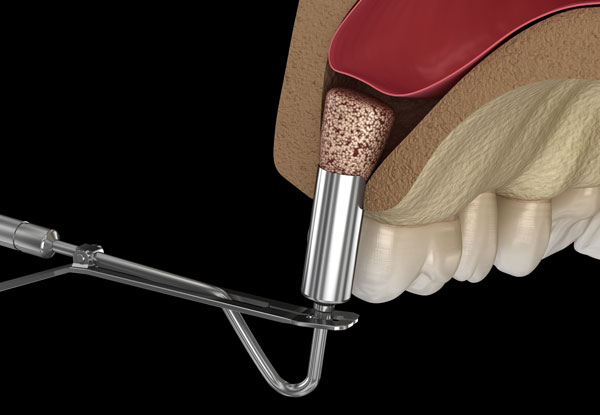
The subantral grafting procedure is performed by making a small window in the sinus above the roots of the maxillary (upper jaw) teeth. The integrity of the membrane lining the sinus is not violated but instead is teased upward to form a small cavity or balloon like space that can be filled with bovine bone (BioOss). A period of six to nine months is required for this bone to consolidate after having formed a scaffold for natural bone replacement. As this procedure relates to placing implants, there are two possibilities.
Immediate Implant Placement with Subantral Grafting
The ability to place implants at the time of the subantral graft is determined by the amount of native bone present between the sinus and the oral cavity. If less than five millimeters of bone is present and the existing bone in the area is soft, it becomes difficult to primarily stabilize the implants at the time of surgery and insure their stability during the period required for graft consolidation. This can result in either an implant failure or a poorly angulated implant. However, if more than five millimeters of bone is present in the above circumstance, the implants can often be placed at the same time as the graft and the bone allowed to consolidate around the implants during the ensuing months. This obviously has the benefit of eliminating a surgical stage as well as shortening the timeline required to bring the implants into function with teeth. When implants are placed at the time of subantral grafting, a consolidation period of usually four to six months is required before the restorative dentist can begin working on building your teeth.
Delayed Implant Placement with Primary Subantral Grafting
If there is inadequate native bone present at the time of subantral grafting for the placement of implants simultaneously, the graft is typically placed as a lone procedure and the site is allowed to mature for several months. Your surgeon will then return at a second stage, when he has deemed that the time period has been sufficient to place the implants. Since the graft has undergone consolidation at that point, only a standard period of implant integration is required after the second stage before your restorative dentist can begin to reconstruct your implants with teeth.
In summary, it is likely that when considering dental implants for the replacement of missing teeth that you will be asked to consider some form of “grafting” to accompany this process. Your doctor will discuss with you which of these procedures that he recommends and why. Furthermore, he can answer questions that you may have regarding the perioperative experience and the post-operative convalescence. All of these procedures are performed very comfortably in an outpatient setting with either local anesthesia or intravenous sedation.